INTRODUCTION
The primary reason children refuse medicine is taste. Bitterness, astringency, and metallic aftertaste cause patients to stop taking their medication altogether. In pharmaceutical development, a medicine that is not taken consistently does not produce the intended therapeutic outcome.
Taste masking is frequently treated as a finishing step rather than a core design consideration. When a palatability problem is discovered late in development, it forces a complete reformulation. That reformulation delays the product launch and adds cost that was not planned for a problem that should have been addressed from the start.
At Vikram Thermo, we have worked on taste masking formulations for over 40 years across paediatric suspensions, orally disintegrating tablets, and liquid oral generics for manufacturers in 45+ countries. The problems that surface in this area follow a consistent pattern, and so do the solutions.
WHAT IS TASTE MASKING?
An active pharmaceutical ingredient, or API, is the drug molecule responsible for the therapeutic effect. Most APIs are inherently bitter because their molecular structure directly activates bitter taste receptors on the tongue. This is not a formulation flaw. It is a molecular property of the compound.
Taste masking prevents that activation. The drug must not come into free contact with taste receptors while the dosage form is in the mouth. After swallowing, the drug must release completely and absorb normally. The masking functions only in the oral cavity and cannot impede drug release in the gastrointestinal tract.
That is the constraint. Effective in the mouth. Desire drug release after swallowing. Getting both right is the formulation challenge.
WHY IT MATTERS
Children are the most significant population for taste masking. Medication refusal in paediatric patients is caused directly by taste. The WHO identifies poor palatability as the primary reason children do not take their medication, and both the FDA and EMA require palatability evaluation as part of paediatric formulation submissions.
Oral suspensions and syrups are the preferred formats for young children. They are also the hardest formats to address, because the drug is already dissolved or dispersed in the liquid. Drug-saliva contact is at its maximum. A polymer coating designed for a solid tablet does not apply in this format.
Orally disintegrating tablets, known as ODTs, dissolve on the tongue within seconds. This makes them useful for patients who cannot swallow conventional tablets. Without taste masking, however, the drug releases into saliva before swallowing. The clinical benefit the format was designed to provide is cancelled by the sensory experience.
In generic drug development, palatability failures can emerge during bioequivalence studies when a coating system or excipient is changed. Even when the bioavailability data is equivalent to the reference product, formulation changes can alter how much drug reaches saliva. A palatability failure at that stage requires reformulation and restarts part of the development timeline.
THE MAIN APPROACHES
No single method applies to all drugs and all dosage forms. Selection depends on the drug's charge at physiological pH, the intended dosage form, the target patient population, and manufacturing capability.
Polymer Film Coating
Polymer film coating is the standard approach for solid dosage forms. A thin polymer layer is applied to the tablet or drug particle, forming a physical barrier between the drug surface and saliva. The polymer must be insoluble at salivary pH, approximately 6.8 to 7.4, so it does not dissolve before the product is swallowed. After swallowing, it must allow drug release at gastric pH, which is below 5.
Our DRUGCOAT® E Series, based on amino methacrylate copolymers, is designed specifically for this application. It dissolves below pH 5, masking bitterness in the oral cavity while releasing the API rapidly once the product reaches the stomach. It is available as granules (E100), powder (EPO), and organic solution (E12.5), giving formulators the flexibility to match processing requirements. At low coating weights, these taste masking coating polymers function as oral barriers. At higher coating weights, the same family can extend drug release, which is why the same polymer chemistry appears in both taste masking and sustained release formulation work.
Aqueous film coating systems, where the polymer is dispersed in water rather than an organic solvent, are standard in commercial pharmaceutical manufacturing. Our DRCOAT® range provides HPMC-based and PVA-based aqueous options for immediate release applications where taste masking is one requirement alongside others.
Ion Exchange Resin Complexation
Ion exchange resin complexation is the primary approach for liquid oral dosage forms where film coating is not applicable.
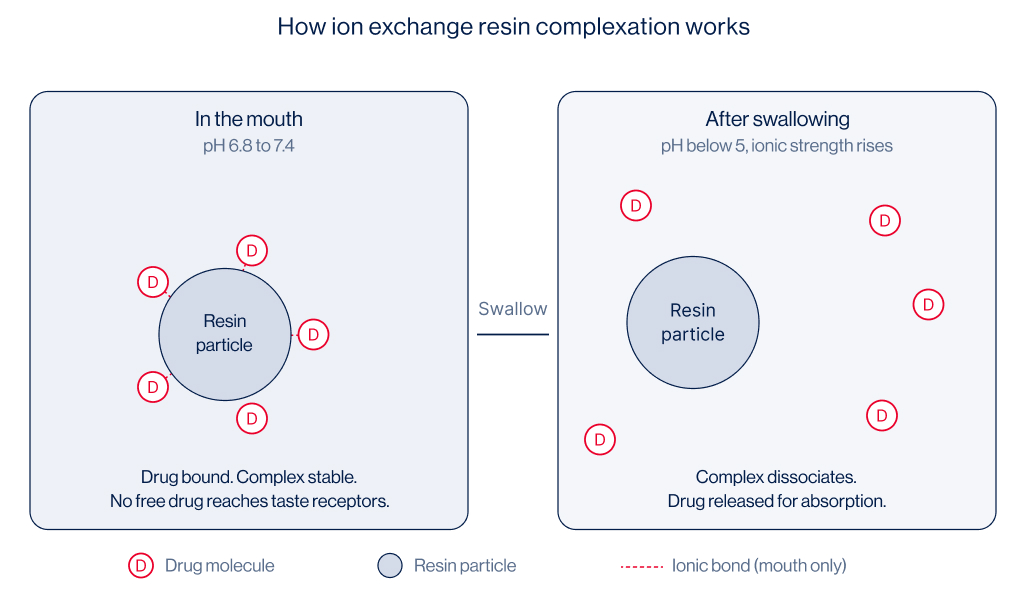
An ion exchange resin is an insoluble polymer particle with charged sites on its surface. When a drug carrying a charge is mixed with the resin in water under controlled pH conditions, the drug binds to the resin through ionic interaction.
The resulting drug-resin complex, called a resinate, is stable in water and in saliva. The drug cannot dissolve freely, so it cannot reach taste receptors. After swallowing, the higher ionic concentration in the gastrointestinal tract causes the complex to break apart, releasing the drug for absorption.
Our APION® T Series is developed specifically for taste masking resin applications in oral suspensions and liquid dosage forms. The series uses carefully selected resin types matched to the drug's ionisation profile at physiological pH. Cation exchange resins are used for basic drugs that carry a positive charge. Anion exchange resins are used for acidic drugs that carry a negative charge. An incorrect selection results in poor binding and no masking effect.
Pharmaceutical grade ion exchange resins have been used in paediatric suspensions for antibiotics, antihistamines, and antitussives for decades. The mechanism is well characterised from a regulatory standpoint, and our APION® T Series is supported by the technical documentation required for global submissions.
Microencapsulation
Microencapsulation surrounds individual drug particles with a coating material at the microscale. The encapsulated particles are incorporated into tablets, capsules, sachets, or suspensions. This approach is compatible with sustained release design when required. Processing routes such as spray congealing and fluid bed coating at very small particle sizes are more technically demanding than standard tablet coating and must be factored into scale-up planning.
Flavours and Sweeteners
Flavours and sweeteners do not mask taste through a physical or chemical mechanism. They modify the sensory environment. For drugs with mild bitterness, flavour selection may be adequate. For drugs with intense, receptor-mediated bitterness, flavours alone are insufficient. The bitter signal from taste receptors overrides the flavour contribution. Flavours are most effective when used to support an already effective taste masking coating system, not to substitute for one.
HOW THE PROCESS WORKS
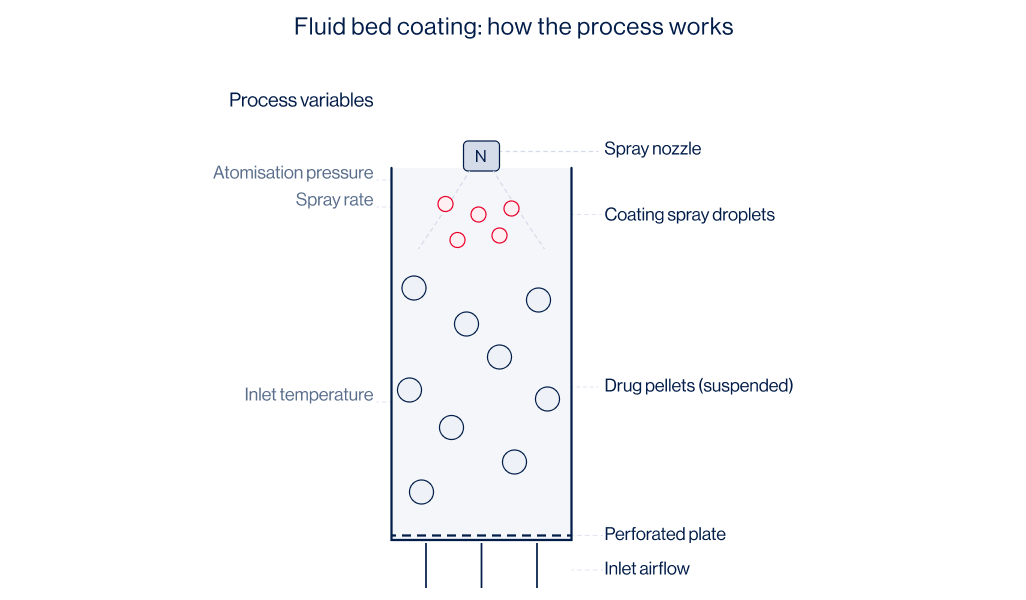
In fluid bed coating, drug pellets or granules are suspended in an upward airstream while a coating dispersion is sprayed onto the surface. The polymer forms a film as water or solvent evaporates. Spray rate, inlet air temperature, atomisation pressure, and particle fluidisation all affect film quality. A spray rate too high relative to drying capacity results in poor film formation. Atomisation pressure determines droplet size, which controls how the polymer spreads on the particle surface before drying.
For ion exchange resin systems, the process is chemical. The drug and resin are combined in aqueous solution at a controlled pH and temperature until the binding reaction reaches equilibrium. The loaded resin is filtered, washed, and either dried or suspended in the product vehicle. Drug loading efficiency is the percentage of the drug actually bound to the resin. It determines dose accuracy in the finished product and is the critical quality attribute to establish at development stage and maintain at commercial scale.
APPLICATIONS BY DOSAGE FORM
COMMON CHALLENGES
In ODT formulations, coating damage during tablet compression is the most frequent failure. The granules are correctly coated, but compression force fractures the film. The drug surface becomes exposed, dissolves in saliva during tablet disintegration, and the patient experiences the bitterness directly. The coating must be mechanically strong enough to survive compression forces, not just chemically effective as a barrier. Both requirements must be addressed together during formulation development.
In resin-based suspension formulations, inconsistent drug loading is the most common cause of batch failures. Poorly controlled pH during complexation, variable contact time, or inconsistency between resin lots results in batches where the drug bound to the resin differs from the target. Because drug loading determines dose accuracy, it requires tight process control throughout manufacturing.
Film cracking during storage is typically caused by insufficient plasticiser in the coating formulation. Coating films must accommodate small physical changes in the tablet over time, including moisture uptake, temperature fluctuation, and minor dimensional changes in the core. A film without adequate plasticiser becomes brittle and cracks, creating pathways for unintended drug dissolution.
FORMULATION INSIGHTS
Taste evaluation should be conducted early. Bitterness is a molecular property of the drug and can be assessed during candidate characterisation. Knowing the bitterness profile at that stage allows the formulation team to select a masking approach before the dosage form is finalised, rather than retrofitting a solution after a clinical palatability failure.
For polymer coating, the pH at which the polymer dissolves or becomes permeable must match the intended site of drug release. A polymer that does not hold at oral pH provides no taste masking. A polymer that does not release at gastric pH prevents the drug from absorbing.
For resin-based systems, the stability of the drug-resin complex must be confirmed across the full shelf life of the product. The suspension vehicle pH and ionic composition must be maintained within specification throughout storage.
At Vikram Thermo, our formulation support teams work with manufacturers at the development stage to select the right approach for the specific drug and dosage form, and to generate the technical data needed for regulatory submissions, from drug loading protocols to dissolution data under simulated oral and gastric conditions.
COMPARISON TABLE: POLYMER COATING VS ION EXCHANGE RESIN
FREQUENTLY ASKED QUESTIONS
1. Is taste masking the same as enteric coating?
No. Enteric coating prevents drug release in the stomach and allows release in the intestine. Taste masking prevents drug dissolution in the mouth. Some polymers can serve both functions at different coat weights, but the performance requirements are different. A taste masking coat must hold for under a minute. An enteric coat must resist gastric conditions for at least two hours.
2. Can taste masking affect bioavailability?
It can if the coating does not dissolve or become permeable after swallowing. In vitro dissolution testing under simulated gastric conditions is required for any taste-masked solid dosage form. Our DRUGCOAT® E Series formulations are characterised for dissolution across pH conditions, and we provide this data as part of standard technical documentation.
3. Are resin-based systems suitable for all APIs?
No. Ion exchange complexation requires the drug to carry a charge at physiological pH. Drugs that are neutral in solution do not bind to the resin effectively. Our team evaluates the drug's ionisation profile before recommending APION® T Series, and where resin complexation is not suitable, we identify the appropriate alternative approach.
4. How early in development should taste masking be considered?
Early enough to influence the choice of dosage form. Bitterness can be assessed during candidate characterisation. Knowing the profile at that stage allows the formulation team to design the product around it from the beginning. We support this evaluation as part of our formulation partnership approach.
5. What regulatory documentation is required for resin-based systems?
A drug master file for the resin material, drug-resin compatibility data, drug loading protocols, stability data for the complex, and in vitro dissolution data under conditions that simulate oral residence and gastric transit. Our APION® T Series is supported by the necessary regulatory documentation for global submissions.
CONCLUSION
Taste masking is a formulation requirement with direct consequences for patient adherence and treatment outcomes. The mechanisms are established and the materials exist. The challenge is identifying the need early, selecting the right approach for the specific drug and dosage form, and maintaining process control through manufacturing and storage.
At Vikram Thermo, this is work we have done for over 40 years across 45+ countries, matching the right polymer or resin system to the formulation problem, and supporting manufacturers from development through commercial scale. Our APION® T Series and DRUGCOAT® E Series represent four decades of learning in this category, backed by EXCiPACT GMP certification, US DMF registration, and WHO cGMP compliance.
For paediatric formulations, this is not a secondary consideration. A child who refuses medication because of its taste is a treatment failure that formulation science had the means to prevent.
Have a Formulation Challenge? Talk to Us.
Taste masking problems rarely arrive with straightforward answers. The right approach depends on the drug, the dosage form, the patient, and the manufacturing process available to you.
If you are working on a bitter API, developing a paediatric suspension, or trying to make an ODT that patients will actually accept, we are ready to have that conversation. Tell us what you are trying to solve. We will tell you honestly whether we can help.
Write to us at contact@vikramthermo.com
%201.jpg)
INTRODUCTION
The primary reason children refuse medicine is taste. Bitterness, astringency, and metallic aftertaste cause patients to stop taking their medication altogether. In pharmaceutical development, a medicine that is not taken consistently does not produce the intended therapeutic outcome.
Taste masking is frequently treated as a finishing step rather than a core design consideration. When a palatability problem is discovered late in development, it forces a complete reformulation. That reformulation delays the product launch and adds cost that was not planned for a problem that should have been addressed from the start.
At Vikram Thermo, we have worked on taste masking formulations for over 40 years across paediatric suspensions, orally disintegrating tablets, and liquid oral generics for manufacturers in 45+ countries. The problems that surface in this area follow a consistent pattern, and so do the solutions.
WHAT IS TASTE MASKING?
An active pharmaceutical ingredient, or API, is the drug molecule responsible for the therapeutic effect. Most APIs are inherently bitter because their molecular structure directly activates bitter taste receptors on the tongue. This is not a formulation flaw. It is a molecular property of the compound.
Taste masking prevents that activation. The drug must not come into free contact with taste receptors while the dosage form is in the mouth. After swallowing, the drug must release completely and absorb normally. The masking functions only in the oral cavity and cannot impede drug release in the gastrointestinal tract.
That is the constraint. Effective in the mouth. Desire drug release after swallowing. Getting both right is the formulation challenge.
WHY IT MATTERS
Children are the most significant population for taste masking. Medication refusal in paediatric patients is caused directly by taste. The WHO identifies poor palatability as the primary reason children do not take their medication, and both the FDA and EMA require palatability evaluation as part of paediatric formulation submissions.
Oral suspensions and syrups are the preferred formats for young children. They are also the hardest formats to address, because the drug is already dissolved or dispersed in the liquid. Drug-saliva contact is at its maximum. A polymer coating designed for a solid tablet does not apply in this format.
Orally disintegrating tablets, known as ODTs, dissolve on the tongue within seconds. This makes them useful for patients who cannot swallow conventional tablets. Without taste masking, however, the drug releases into saliva before swallowing. The clinical benefit the format was designed to provide is cancelled by the sensory experience.
In generic drug development, palatability failures can emerge during bioequivalence studies when a coating system or excipient is changed. Even when the bioavailability data is equivalent to the reference product, formulation changes can alter how much drug reaches saliva. A palatability failure at that stage requires reformulation and restarts part of the development timeline.
THE MAIN APPROACHES
No single method applies to all drugs and all dosage forms. Selection depends on the drug's charge at physiological pH, the intended dosage form, the target patient population, and manufacturing capability.
Polymer Film Coating
Polymer film coating is the standard approach for solid dosage forms. A thin polymer layer is applied to the tablet or drug particle, forming a physical barrier between the drug surface and saliva. The polymer must be insoluble at salivary pH, approximately 6.8 to 7.4, so it does not dissolve before the product is swallowed. After swallowing, it must allow drug release at gastric pH, which is below 5.
Our DRUGCOAT® E Series, based on amino methacrylate copolymers, is designed specifically for this application. It dissolves below pH 5, masking bitterness in the oral cavity while releasing the API rapidly once the product reaches the stomach. It is available as granules (E100), powder (EPO), and organic solution (E12.5), giving formulators the flexibility to match processing requirements. At low coating weights, these taste masking coating polymers function as oral barriers. At higher coating weights, the same family can extend drug release, which is why the same polymer chemistry appears in both taste masking and sustained release formulation work.
Aqueous film coating systems, where the polymer is dispersed in water rather than an organic solvent, are standard in commercial pharmaceutical manufacturing. Our DRCOAT® range provides HPMC-based and PVA-based aqueous options for immediate release applications where taste masking is one requirement alongside others.
Ion Exchange Resin Complexation
Ion exchange resin complexation is the primary approach for liquid oral dosage forms where film coating is not applicable.
An ion exchange resin is an insoluble polymer particle with charged sites on its surface. When a drug carrying a charge is mixed with the resin in water under controlled pH conditions, the drug binds to the resin through ionic interaction.
The resulting drug-resin complex, called a resinate, is stable in water and in saliva. The drug cannot dissolve freely, so it cannot reach taste receptors. After swallowing, the higher ionic concentration in the gastrointestinal tract causes the complex to break apart, releasing the drug for absorption.
Our APION® T Series is developed specifically for taste masking resin applications in oral suspensions and liquid dosage forms. The series uses carefully selected resin types matched to the drug's ionisation profile at physiological pH. Cation exchange resins are used for basic drugs that carry a positive charge. Anion exchange resins are used for acidic drugs that carry a negative charge. An incorrect selection results in poor binding and no masking effect.
Pharmaceutical grade ion exchange resins have been used in paediatric suspensions for antibiotics, antihistamines, and antitussives for decades. The mechanism is well characterised from a regulatory standpoint, and our APION® T Series is supported by the technical documentation required for global submissions.
Microencapsulation
Microencapsulation surrounds individual drug particles with a coating material at the microscale. The encapsulated particles are incorporated into tablets, capsules, sachets, or suspensions. This approach is compatible with sustained release design when required. Processing routes such as spray congealing and fluid bed coating at very small particle sizes are more technically demanding than standard tablet coating and must be factored into scale-up planning.
Flavours and Sweeteners
Flavours and sweeteners do not mask taste through a physical or chemical mechanism. They modify the sensory environment. For drugs with mild bitterness, flavour selection may be adequate. For drugs with intense, receptor-mediated bitterness, flavours alone are insufficient. The bitter signal from taste receptors overrides the flavour contribution. Flavours are most effective when used to support an already effective taste masking coating system, not to substitute for one.
HOW THE PROCESS WORKS
In fluid bed coating, drug pellets or granules are suspended in an upward airstream while a coating dispersion is sprayed onto the surface. The polymer forms a film as water or solvent evaporates. Spray rate, inlet air temperature, atomisation pressure, and particle fluidisation all affect film quality. A spray rate too high relative to drying capacity results in poor film formation. Atomisation pressure determines droplet size, which controls how the polymer spreads on the particle surface before drying.
For ion exchange resin systems, the process is chemical. The drug and resin are combined in aqueous solution at a controlled pH and temperature until the binding reaction reaches equilibrium. The loaded resin is filtered, washed, and either dried or suspended in the product vehicle. Drug loading efficiency is the percentage of the drug actually bound to the resin. It determines dose accuracy in the finished product and is the critical quality attribute to establish at development stage and maintain at commercial scale.
APPLICATIONS BY DOSAGE FORM
COMMON CHALLENGES
In ODT formulations, coating damage during tablet compression is the most frequent failure. The granules are correctly coated, but compression force fractures the film. The drug surface becomes exposed, dissolves in saliva during tablet disintegration, and the patient experiences the bitterness directly. The coating must be mechanically strong enough to survive compression forces, not just chemically effective as a barrier. Both requirements must be addressed together during formulation development.
In resin-based suspension formulations, inconsistent drug loading is the most common cause of batch failures. Poorly controlled pH during complexation, variable contact time, or inconsistency between resin lots results in batches where the drug bound to the resin differs from the target. Because drug loading determines dose accuracy, it requires tight process control throughout manufacturing.
Film cracking during storage is typically caused by insufficient plasticiser in the coating formulation. Coating films must accommodate small physical changes in the tablet over time, including moisture uptake, temperature fluctuation, and minor dimensional changes in the core. A film without adequate plasticiser becomes brittle and cracks, creating pathways for unintended drug dissolution.
FORMULATION INSIGHTS
Taste evaluation should be conducted early. Bitterness is a molecular property of the drug and can be assessed during candidate characterisation. Knowing the bitterness profile at that stage allows the formulation team to select a masking approach before the dosage form is finalised, rather than retrofitting a solution after a clinical palatability failure.
For polymer coating, the pH at which the polymer dissolves or becomes permeable must match the intended site of drug release. A polymer that does not hold at oral pH provides no taste masking. A polymer that does not release at gastric pH prevents the drug from absorbing.
For resin-based systems, the stability of the drug-resin complex must be confirmed across the full shelf life of the product. The suspension vehicle pH and ionic composition must be maintained within specification throughout storage.
At Vikram Thermo, our formulation support teams work with manufacturers at the development stage to select the right approach for the specific drug and dosage form, and to generate the technical data needed for regulatory submissions, from drug loading protocols to dissolution data under simulated oral and gastric conditions.
COMPARISON TABLE: POLYMER COATING VS ION EXCHANGE RESIN
FREQUENTLY ASKED QUESTIONS
1. Is taste masking the same as enteric coating?
No. Enteric coating prevents drug release in the stomach and allows release in the intestine. Taste masking prevents drug dissolution in the mouth. Some polymers can serve both functions at different coat weights, but the performance requirements are different. A taste masking coat must hold for under a minute. An enteric coat must resist gastric conditions for at least two hours.
2. Can taste masking affect bioavailability?
It can if the coating does not dissolve or become permeable after swallowing. In vitro dissolution testing under simulated gastric conditions is required for any taste-masked solid dosage form. Our DRUGCOAT® E Series formulations are characterised for dissolution across pH conditions, and we provide this data as part of standard technical documentation.
3. Are resin-based systems suitable for all APIs?
No. Ion exchange complexation requires the drug to carry a charge at physiological pH. Drugs that are neutral in solution do not bind to the resin effectively. Our team evaluates the drug's ionisation profile before recommending APION® T Series, and where resin complexation is not suitable, we identify the appropriate alternative approach.
4. How early in development should taste masking be considered?
Early enough to influence the choice of dosage form. Bitterness can be assessed during candidate characterisation. Knowing the profile at that stage allows the formulation team to design the product around it from the beginning. We support this evaluation as part of our formulation partnership approach.
5. What regulatory documentation is required for resin-based systems?
A drug master file for the resin material, drug-resin compatibility data, drug loading protocols, stability data for the complex, and in vitro dissolution data under conditions that simulate oral residence and gastric transit. Our APION® T Series is supported by the necessary regulatory documentation for global submissions.
CONCLUSION
Taste masking is a formulation requirement with direct consequences for patient adherence and treatment outcomes. The mechanisms are established and the materials exist. The challenge is identifying the need early, selecting the right approach for the specific drug and dosage form, and maintaining process control through manufacturing and storage.
At Vikram Thermo, this is work we have done for over 40 years across 45+ countries, matching the right polymer or resin system to the formulation problem, and supporting manufacturers from development through commercial scale. Our APION® T Series and DRUGCOAT® E Series represent four decades of learning in this category, backed by EXCiPACT GMP certification, US DMF registration, and WHO cGMP compliance.
For paediatric formulations, this is not a secondary consideration. A child who refuses medication because of its taste is a treatment failure that formulation science had the means to prevent.
Have a Formulation Challenge? Talk to Us.
Taste masking problems rarely arrive with straightforward answers. The right approach depends on the drug, the dosage form, the patient, and the manufacturing process available to you.
If you are working on a bitter API, developing a paediatric suspension, or trying to make an ODT that patients will actually accept, we are ready to have that conversation. Tell us what you are trying to solve. We will tell you honestly whether we can help.
Write to us at contact@vikramthermo.com

.jpg)
- Venue:
- Date:
- Booth:
- Time:
- Hosted by:
- Venue:
- Date:
- Booth:
- Time:
- Hosted by: