
.jpg)
Immediate Release vs Sustained Release Tablets: Which Drug Delivery Strategy Is Right for Your Formulation?
The formulation decision comes before the coating decision. Most of the time, it comes well before it.
We have supported formulation development across 45+ countries since 1985. The conversations that take longest to resolve are rarely about which polymer to use. They are about which release strategy was right for this drug, this patient population and this manufacturing environment. A formulator who walks into a polymer selection conversation without a clear answer to that question is working in the wrong order.
Whether a tablet should release its active pharmaceutical ingredient immediately or sustain it over hours is not a coating question. It is a clinical question first, then a pharmacokinetic question, then a manufacturing question. Formulators who treat it as a pharmaceutical coating polymers selection question find out the hard way. In dissolution studies that cannot meet spec. In stability data that drifts. In regulatory submissions that require justification for a choice that was never properly made.
This article works through how that decision is made. Not in abstract terms. In the terms a formulator actually needs.
The United States Pharmacopeia standard sets immediate vs sustained release formulations apart at the first step: immediate release requires dissolution of not less than 85% of the labelled drug amount within 30 minutes. That number has consequences. It means the coating on an immediate release tablet, if there is one, cannot contribute to the release profile. Its job is protection: appearance, moisture, taste. Not control.
Paracetamol. Ibuprofen. Most antibiotics. Immediate release by design, not by default. The pharmacology demands fast onset and that is what it gets.
But there is a cost to fast onset that formulation teams sometimes discover later than they should. Peak plasma concentrations are high. They fall sharply. With some drugs the peak itself is the clinical problem. Gastrointestinal irritation, cardiovascular side effects, central nervous system effects that are concentration-dependent rather than dose-dependent. A patient on a four-times-daily analgesic who experiences nausea at every dose is experiencing the immediate release peak, not the drug. That distinction matters when the formulation strategy is still open.
Sustained release does not automatically solve this. But it does remove the peak. The sustained release formulator is designing a different pharmacokinetic shape: a slower rise, a longer plateau, a gentler decline. Whether that shape is clinically better depends entirely on the drug and the patient. Not on the polymer.

Sustained release is not one technology. It is an outcome, achieved through mechanisms that are quite different from each other and that require different functional excipients pharmaceutical decisions.
Membrane-controlled release works through a polymer film that does not dissolve. Drug diffuses through it at a rate determined by the membrane's permeability. Ammonio methacrylate copolymer, the chemistry behind DRUGCOAT® RL and RS Series, has pH-independent solubility and low water permeability. This is how tablet coating works in a sustained release context: the film controls diffusion rather than dissolving. RL100 is more permeable than RS100 because it carries more quaternary ammonium groups. Most formulations use a ratio of the two to hit a specific release target rather than one grade alone.
Matrix-controlled release embeds the drug in a polymer matrix (hydroxypropyl methylcellulose being the most common) and releases it as fluid penetrates and the polymer swells or erodes. No separate film. No curing step. Operationally more accessible for many manufacturers, which matters more than people acknowledge at the formulation planning stage.
Osmotic systems are a third option that rarely comes up in generic development. Elegant in principle. The manufacturing complexity and cost put them out of reach for most.
The polymer choice follows the mechanism choice. Not the other way around. This seems obvious. It is consistently not how the conversation starts.
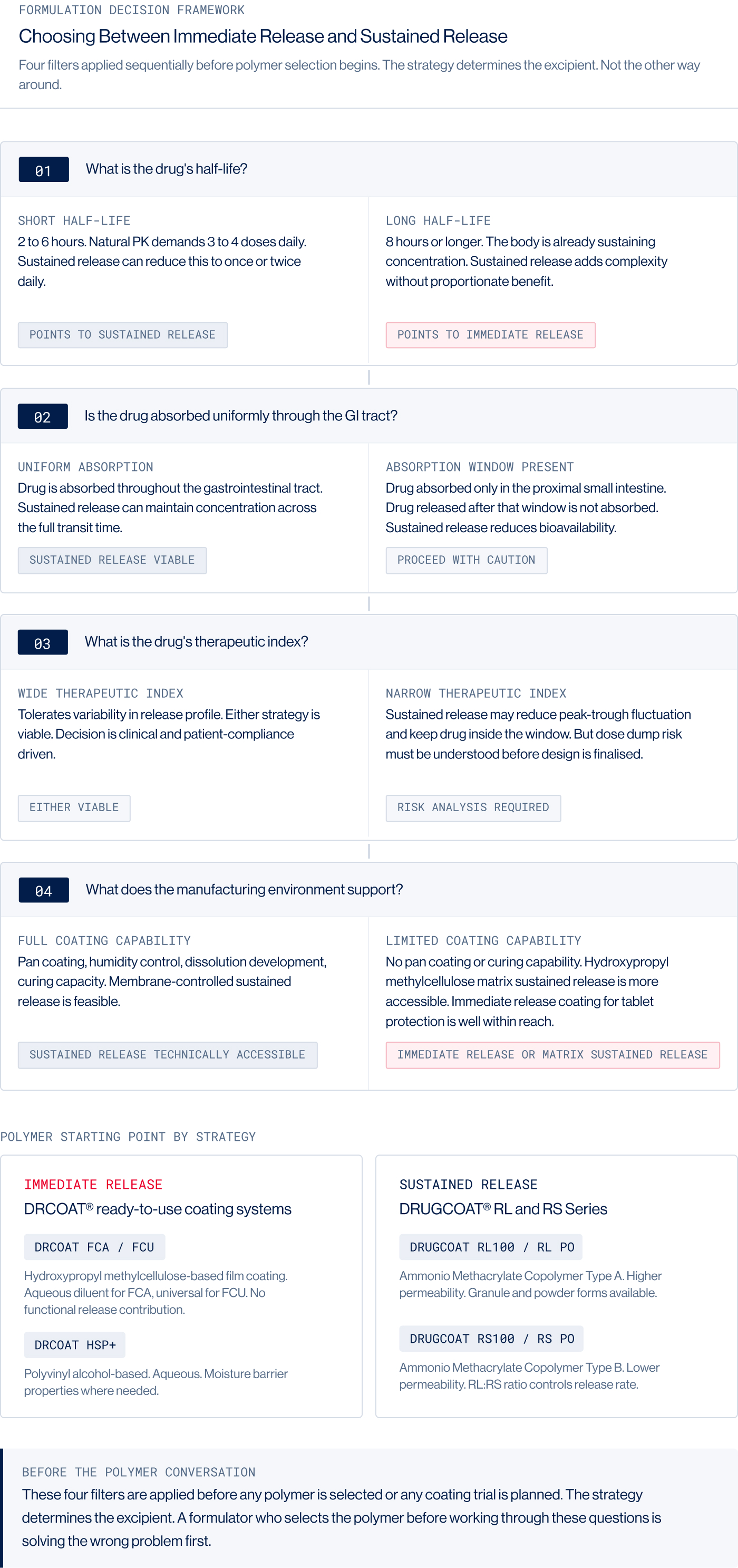
Half-life is where the strategy question begins. A drug with a half-life of eight hours or more is often not a strong candidate for sustained release. The body is already doing the work. A drug with a half-life of two to four hours, requiring three or four doses daily to maintain levels, is where sustained release earns its place. Once daily is a genuine patient benefit when the alternative is setting an alarm for 3am.
The absorption window is where formulators get caught out more often. A drug absorbed only in the proximal small intestine has two to four hours in that segment. Drug released after that window is excreted, not absorbed. Sustained release in this situation does not improve bioavailability. It reduces it. Metformin is the most cited example. Formulated successfully as a sustained release coating polymer product, but only by teams who designed the release profile to work within the absorption window rather than assuming uniform gastrointestinal absorption.
Therapeutic index is where the risk analysis lives. Narrow therapeutic index drugs are not automatically unsuitable for sustained release. Sometimes sustained release is precisely the tool to reduce peak-trough fluctuation and keep a drug inside a tight window. But the failure mode has to be understood before the design is committed. If a coating fails and the full 12-hour dose releases immediately, what happens? Some drugs tolerate it. Some do not. This is not a question to answer at the stability review.
Manufacturing environment is the question that most often overrides the others in practice. A formulator can design the perfect membrane-controlled sustained release coating polymer product for a manufacturer who does not have a humidity-controlled coating suite, adequate coating pan experience or in-house dissolution development capability. The formulation will not survive contact with the process. hydroxypropyl methylcellulose matrix is more accessible and for many situations it is the right starting point for that reason alone. DRUGCOAT® RL and RS Series come in granule form (RL100, RS100), powder form (RLPO, RSPO) and organic solution (RL12.5, RS12.5). Different forms for different process capabilities. But curing is non-negotiable regardless of form. Films applied from dispersion must be held at controlled temperature and humidity after coating to allow full polymer coalescence. Skipping curing because the schedule is tight is one of the most consistent causes of sustained release failure at scale. We see this regularly.
Where the two strategies differ: a practical comparison
When immediate release is the right answer
Sustained release is not automatically superior. There are drugs where it offers no clinical advantage, where the formulation complexity is unjustified and where a well-executed immediate release product is simply the better decision.
Antibiotics that require sustained high tissue concentration and rapid bactericidal action. Analgesics for acute breakthrough pain. Drugs metabolised to active metabolites in a first-pass-dependent way that sustained release disrupts. Drugs with very narrow absorption windows where extending release reduces bioavailability rather than improving it.
In these situations immediate release is not a limitation. DRCOAT® FCA or FCU, hydroxypropyl methylcellulose-based ready-to-use tablet coating system, delivers a consistent immediate release coating polymer without the process complexity of functional polymer films. The clinical decision comes first. The product follows.
Frequently asked questions
1. Can a drug be formulated as both immediate release and sustained release in the same tablet?
Yes. Bilayer tablet technology and reservoir-core designs allow an immediate release loading dose in one layer and a sustained release component in another. The immediate release fraction establishes plasma concentration quickly. The sustained release fraction maintains it. The formulation complexity of these systems is significantly higher than either format alone.
2. Does sustained release always mean better patient compliance?
Not automatically. Once-daily dosing improves adherence for chronic conditions where the patient manages their own medication over months or years. For short-course treatments, a five-day antibiotic course for instance, the compliance benefit is less meaningful. The decision has to be grounded in the actual treatment context.
3. How do we establish the dissolution method for a sustained release product?
Sustained release dissolution methods require more development than immediate release methods. The medium, apparatus type, agitation speed and time points all need justification. For regulated markets, in vitro/in vivo correlation may be required. This is a significant development resource commitment and needs to be planned into the project timeline from the beginning.
4. What curing conditions are recommended for DRUGCOAT® RL and RS coatings?
Curing conditions are product and process specific. As a general starting point, 40°C with 75% relative humidity for a minimum of 24 hours is common for aqueous-applied ammonio methacrylate copolymer films. Final protocols should be established through dissolution studies comparing pre-cured and post-cured profiles, with stability confirmation at accelerated conditions. We provide curing protocol guidance as standard.
5. Is sustained release development always more expensive?
Development cost is higher. Polymer costs are higher. Process and dissolution method development take more time. Whether the investment is justified depends on the commercial context: patent strategy, competitive differentiation, compliance data requirements or regulatory market expectations. For some drugs the economics are compelling. For others, a well-executed immediate release product is the right business decision.
Conclusion
The release strategy decision shapes everything that follows. Excipients, process, dissolution methodology, stability programme, regulatory pathway. All of it flows from this one early choice. Making it on the basis of clinical pharmacology and manufacturing reality, rather than instinct or what a competitor did, reduces the cost of development substantially.
We are India's first EXCiPACT GMP-certified tablet coating polymer manufacturer, established 1985. US DMF registration and WHO cGMP compliance are in place across our DRUGCOAT® and DRCOAT® families. For sustained release coating: DRUGCOAT® RL and RS Series. For immediate release coating: DRCOAT® FCA, FCU and the full film coating polymer for tablets immediate release range. The polymer choice is downstream of the formulation strategy. Get the strategy right first.
Choosing Between Immediate Release and Sustained Release for Your Next Product? Talk to Us.
Tell us the drug, the indication, the dosing frequency target and the manufacturing context. We will tell you which release mechanism fits, which polymer family to start with and what documentation is available before your first trial batch.
Write to us at contact@vikramthermo.com
%201.jpg)
Immediate Release vs Sustained Release Tablets: Which Drug Delivery Strategy Is Right for Your Formulation?
The formulation decision comes before the coating decision. Most of the time, it comes well before it.
We have supported formulation development across 45+ countries since 1985. The conversations that take longest to resolve are rarely about which polymer to use. They are about which release strategy was right for this drug, this patient population and this manufacturing environment. A formulator who walks into a polymer selection conversation without a clear answer to that question is working in the wrong order.
Whether a tablet should release its active pharmaceutical ingredient immediately or sustain it over hours is not a coating question. It is a clinical question first, then a pharmacokinetic question, then a manufacturing question. Formulators who treat it as a pharmaceutical coating polymers selection question find out the hard way. In dissolution studies that cannot meet spec. In stability data that drifts. In regulatory submissions that require justification for a choice that was never properly made.
This article works through how that decision is made. Not in abstract terms. In the terms a formulator actually needs.
The United States Pharmacopeia standard sets immediate vs sustained release formulations apart at the first step: immediate release requires dissolution of not less than 85% of the labelled drug amount within 30 minutes. That number has consequences. It means the coating on an immediate release tablet, if there is one, cannot contribute to the release profile. Its job is protection: appearance, moisture, taste. Not control.
Paracetamol. Ibuprofen. Most antibiotics. Immediate release by design, not by default. The pharmacology demands fast onset and that is what it gets.
But there is a cost to fast onset that formulation teams sometimes discover later than they should. Peak plasma concentrations are high. They fall sharply. With some drugs the peak itself is the clinical problem. Gastrointestinal irritation, cardiovascular side effects, central nervous system effects that are concentration-dependent rather than dose-dependent. A patient on a four-times-daily analgesic who experiences nausea at every dose is experiencing the immediate release peak, not the drug. That distinction matters when the formulation strategy is still open.
Sustained release does not automatically solve this. But it does remove the peak. The sustained release formulator is designing a different pharmacokinetic shape: a slower rise, a longer plateau, a gentler decline. Whether that shape is clinically better depends entirely on the drug and the patient. Not on the polymer.
Sustained release is not one technology. It is an outcome, achieved through mechanisms that are quite different from each other and that require different functional excipients pharmaceutical decisions.
Membrane-controlled release works through a polymer film that does not dissolve. Drug diffuses through it at a rate determined by the membrane's permeability. Ammonio methacrylate copolymer, the chemistry behind DRUGCOAT® RL and RS Series, has pH-independent solubility and low water permeability. This is how tablet coating works in a sustained release context: the film controls diffusion rather than dissolving. RL100 is more permeable than RS100 because it carries more quaternary ammonium groups. Most formulations use a ratio of the two to hit a specific release target rather than one grade alone.
Matrix-controlled release embeds the drug in a polymer matrix (hydroxypropyl methylcellulose being the most common) and releases it as fluid penetrates and the polymer swells or erodes. No separate film. No curing step. Operationally more accessible for many manufacturers, which matters more than people acknowledge at the formulation planning stage.
Osmotic systems are a third option that rarely comes up in generic development. Elegant in principle. The manufacturing complexity and cost put them out of reach for most.
The polymer choice follows the mechanism choice. Not the other way around. This seems obvious. It is consistently not how the conversation starts.
Half-life is where the strategy question begins. A drug with a half-life of eight hours or more is often not a strong candidate for sustained release. The body is already doing the work. A drug with a half-life of two to four hours, requiring three or four doses daily to maintain levels, is where sustained release earns its place. Once daily is a genuine patient benefit when the alternative is setting an alarm for 3am.
The absorption window is where formulators get caught out more often. A drug absorbed only in the proximal small intestine has two to four hours in that segment. Drug released after that window is excreted, not absorbed. Sustained release in this situation does not improve bioavailability. It reduces it. Metformin is the most cited example. Formulated successfully as a sustained release coating polymer product, but only by teams who designed the release profile to work within the absorption window rather than assuming uniform gastrointestinal absorption.
Therapeutic index is where the risk analysis lives. Narrow therapeutic index drugs are not automatically unsuitable for sustained release. Sometimes sustained release is precisely the tool to reduce peak-trough fluctuation and keep a drug inside a tight window. But the failure mode has to be understood before the design is committed. If a coating fails and the full 12-hour dose releases immediately, what happens? Some drugs tolerate it. Some do not. This is not a question to answer at the stability review.
Manufacturing environment is the question that most often overrides the others in practice. A formulator can design the perfect membrane-controlled sustained release coating polymer product for a manufacturer who does not have a humidity-controlled coating suite, adequate coating pan experience or in-house dissolution development capability. The formulation will not survive contact with the process. hydroxypropyl methylcellulose matrix is more accessible and for many situations it is the right starting point for that reason alone. DRUGCOAT® RL and RS Series come in granule form (RL100, RS100), powder form (RLPO, RSPO) and organic solution (RL12.5, RS12.5). Different forms for different process capabilities. But curing is non-negotiable regardless of form. Films applied from dispersion must be held at controlled temperature and humidity after coating to allow full polymer coalescence. Skipping curing because the schedule is tight is one of the most consistent causes of sustained release failure at scale. We see this regularly.
Where the two strategies differ: a practical comparison
When immediate release is the right answer
Sustained release is not automatically superior. There are drugs where it offers no clinical advantage, where the formulation complexity is unjustified and where a well-executed immediate release product is simply the better decision.
Antibiotics that require sustained high tissue concentration and rapid bactericidal action. Analgesics for acute breakthrough pain. Drugs metabolised to active metabolites in a first-pass-dependent way that sustained release disrupts. Drugs with very narrow absorption windows where extending release reduces bioavailability rather than improving it.
In these situations immediate release is not a limitation. DRCOAT® FCA or FCU, hydroxypropyl methylcellulose-based ready-to-use tablet coating system, delivers a consistent immediate release coating polymer without the process complexity of functional polymer films. The clinical decision comes first. The product follows.
Frequently asked questions
1. Can a drug be formulated as both immediate release and sustained release in the same tablet?
Yes. Bilayer tablet technology and reservoir-core designs allow an immediate release loading dose in one layer and a sustained release component in another. The immediate release fraction establishes plasma concentration quickly. The sustained release fraction maintains it. The formulation complexity of these systems is significantly higher than either format alone.
2. Does sustained release always mean better patient compliance?
Not automatically. Once-daily dosing improves adherence for chronic conditions where the patient manages their own medication over months or years. For short-course treatments, a five-day antibiotic course for instance, the compliance benefit is less meaningful. The decision has to be grounded in the actual treatment context.
3. How do we establish the dissolution method for a sustained release product?
Sustained release dissolution methods require more development than immediate release methods. The medium, apparatus type, agitation speed and time points all need justification. For regulated markets, in vitro/in vivo correlation may be required. This is a significant development resource commitment and needs to be planned into the project timeline from the beginning.
4. What curing conditions are recommended for DRUGCOAT® RL and RS coatings?
Curing conditions are product and process specific. As a general starting point, 40°C with 75% relative humidity for a minimum of 24 hours is common for aqueous-applied ammonio methacrylate copolymer films. Final protocols should be established through dissolution studies comparing pre-cured and post-cured profiles, with stability confirmation at accelerated conditions. We provide curing protocol guidance as standard.
5. Is sustained release development always more expensive?
Development cost is higher. Polymer costs are higher. Process and dissolution method development take more time. Whether the investment is justified depends on the commercial context: patent strategy, competitive differentiation, compliance data requirements or regulatory market expectations. For some drugs the economics are compelling. For others, a well-executed immediate release product is the right business decision.
Conclusion
The release strategy decision shapes everything that follows. Excipients, process, dissolution methodology, stability programme, regulatory pathway. All of it flows from this one early choice. Making it on the basis of clinical pharmacology and manufacturing reality, rather than instinct or what a competitor did, reduces the cost of development substantially.
We are India's first EXCiPACT GMP-certified tablet coating polymer manufacturer, established 1985. US DMF registration and WHO cGMP compliance are in place across our DRUGCOAT® and DRCOAT® families. For sustained release coating: DRUGCOAT® RL and RS Series. For immediate release coating: DRCOAT® FCA, FCU and the full film coating polymer for tablets immediate release range. The polymer choice is downstream of the formulation strategy. Get the strategy right first.
Choosing Between Immediate Release and Sustained Release for Your Next Product? Talk to Us.
Tell us the drug, the indication, the dosing frequency target and the manufacturing context. We will tell you which release mechanism fits, which polymer family to start with and what documentation is available before your first trial batch.
Write to us at contact@vikramthermo.com
- Venue:
- Date:
- Booth:
- Time:
- Hosted by:
- Venue:
- Date:
- Booth:
- Time:
- Hosted by: